


The healthcare landscape in the United States is undergoing a profound and irreversible paradigm shift from volume to value. This transformation represents not merely an operational adjustment but a strategic geopolitical shift that demands highly executive leadership. As we navigate this evolving ecosystem, a critical question for every C-suite executive and board member is: What leadership competencies define value-based care excellence? JRG Partners, a premier US-based executive search firm, consistently advises that robust leadership, deeply versed in integrated clinical-financial strategies and adept at navigating complex US regulatory environments, is the linchpin for sustainable value realization in this new era.
Key Strategic Imperatives for Value Realization
The transition to outcome-driven healthcare models necessitates a re-evaluation of organizational purpose and executive mandates. Our analysis identifies several critical strategic imperatives:
- Value-based care (VBC) represents a strategic imperative, demanding proactive executive leadership to cultivate resilient healthcare ecosystems. This is a foundational element of sound corporate governance.
- Successful VBC implementation mandates a seamless integration of clinical-financial strategies, robust data governance, and sophisticated strategic risk management.
- Cultivating physician engagement, aligning incentives, and fostering a patient-centric organizational culture are paramount for driving this transformation and ensuring long-term success.
- Foundational digital infrastructure and advanced analytics are indispensable for scaling, optimizing, and ensuring interoperability within VBC delivery frameworks.
- Executive leaders must master complex contract negotiations, redefine performance metrics, and foster a culture of innovation to successfully scale VBC across entire enterprises.
Shifting from Volume to Value Leadership Mindsets
The journey from a fee-for-service mentality to a value-centric approach requires a fundamental recalibration of leadership philosophy and organizational ethos. Boards must prioritize leaders capable of orchestrating this profound cultural and operational metamorphosis.
- Re-envisioning Organizational Purpose: Defining a clear mission anchored in population health outcomes and holistic well-being, moving beyond episodic treatment.
- Developing New Leadership Competencies: Cultivating C-suite skills in strategic risk management, financial acumen for shared savings models, and cross-functional collaboration across traditionally siloed departments. JRG Partners specializes in identifying and placing executives with proven expertise in these critical areas, understanding the unique demands of the US healthcare market.
- Fostering a Culture of Accountability and Innovation: Empowering multidisciplinary teams to experiment, derive insights from data, and prioritize patient results over service volume. This necessitates a proactive approach to talent development and retention.
- Addressing Stakeholder Resistance: Implementing sophisticated communication strategies to articulate the imperative for change and secure buy-in from clinical, administrative, and financial teams across the enterprise.
Organizations with strong executive sponsorship are 2.5 times more likely to report successful value-based care model implementations.
Risk Stratification and Population Health Governance
Effective population health management is the cornerstone of VBC, demanding sophisticated analytical capabilities and stringent data stewardship to optimize patient care and resource allocation.

- Leveraging Advanced Analytics: Implementing predictive modeling tools for patient segmentation, identifying high-risk populations, and understanding the impact of social determinants of health (SDOH). This proactive stance enables targeted interventions.
- Establishing Robust Data Governance: Creating comprehensive frameworks for secure data acquisition, stringent privacy compliance (e.g., HIPAA in the US), fostering interoperability, and ensuring ethical data use across the continuum of care. This is a non-negotiable fiduciary duty.
- Designing Proactive Care Pathways: Developing targeted interventions and preventative programs for identified at-risk groups to strategically reduce avoidable utilization and improve outcomes.
- Integrating Community Resources: Architecting robust connections between patients and non-clinical support services to holistically address SDOH and advance health equity.
Effective risk stratification can reduce emergency department visits by up to 15% and readmission rates by 10% for high-risk patient cohorts.
Aligning Incentives Across Clinical-Financial Silos
The transition to VBC often falters due to misaligned incentives. Executive leaders must architect innovative compensation and organizational structures that bridge traditional clinical and financial divides, fostering shared accountability and success.
- Designing VBC Compensation Models: Developing innovative remuneration structures that reward quality outcomes, cost efficiency, and patient satisfaction for all stakeholders—from primary care physicians to specialist networks.
- Fostering Interdepartmental Collaboration: Breaking down traditional organizational barriers between clinical departments, finance, operations, and IT through shared strategic goals and transparent reporting mechanisms.
- Implementing Transparent Metrics: Creating shared dashboards and reporting systems to track progress, ensure transparency, and facilitate shared accountability across all levels of the organization.
- Strategic Resource Allocation: Deliberately redirecting investments from legacy fee-for-service infrastructure to essential population health management tools and preventative care initiatives.
Misaligned incentives are cited as a primary barrier by 60% of executives attempting to transition to value-based care models.
Digital Enablement for Care Coordination Scale
Digital infrastructure is not merely supportive; it is foundational to achieving the scale and efficiency required for successful VBC delivery across the US healthcare system. Leaders must invest strategically in platforms that enhance connectivity and actionable insights.
- Telehealth and Remote Patient Monitoring (RPM): Deploying cutting-edge virtual care platforms and RPM devices to extend reach, improve access, and proactively manage chronic conditions across diverse geographies.
- Interoperable Health Information Exchanges (HIEs): Building seamless data flow mechanisms between providers, payers, and community services to create a holistic and actionable patient view.
- AI and Machine Learning for Insights: Utilizing advanced artificial intelligence for predictive analytics, crafting personalized care plans, and identifying care gaps at scale, optimizing resource deployment. We find that executive talent capable of leading such technological integration is highly sought after by our US clients.
- Cybersecurity and Data Integrity: Ensuring robust protection of sensitive patient data across all digital platforms and connected devices, a critical element of governance and trust.
A key strategic consideration is: Which digital platforms accelerate value-based care ROI? The answer lies in platforms that prioritize interoperability, provide real-time data analytics, and seamlessly integrate into existing clinical workflows, ultimately driving efficiency and improving patient outcomes.
Physician Economics in Capitated Environments
Engaging physicians as partners, rather than simply practitioners, is paramount for VBC success. This requires a deep understanding of physician economics and autonomy within new payment structures.
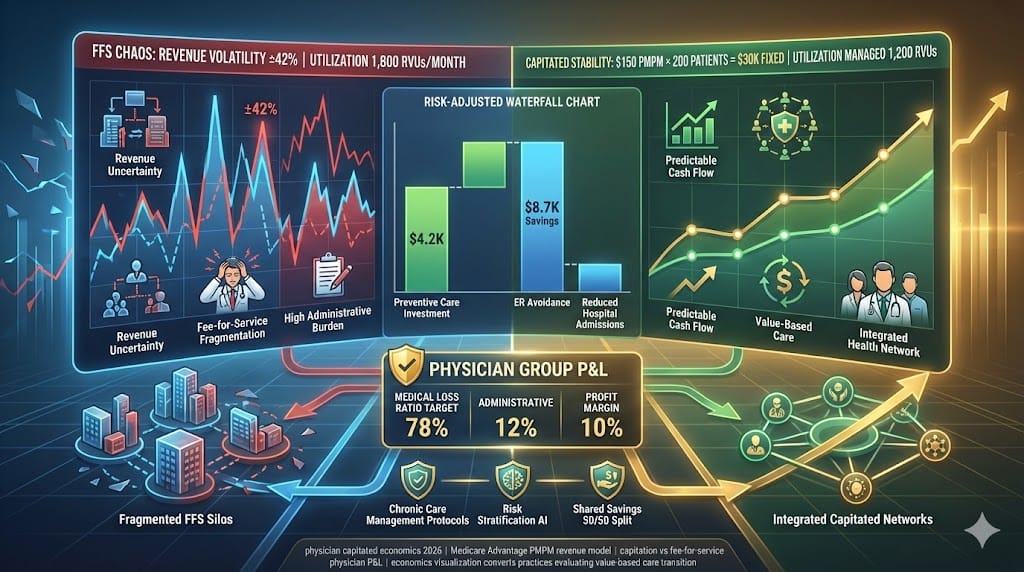
- Educating Physicians on VBC Financials: Providing clear, comprehensive training on new reimbursement models, risk-sharing mechanisms, and the direct impact of quality and cost performance on compensation.
- Developing Fair Compensation Formulas: Designing physician compensation structures that judiciously balance salary, quality bonuses, and transparent shared savings participation, reflecting both individual and collective contributions.
- Support for Practice Transformation: Offering essential resources, administrative support, and technology to help physicians adapt to new workflows, documentation requirements, and performance metrics, mitigating potential burnout.
- Addressing Autonomy and Burnout Concerns: Actively engaging physicians in the design and implementation process to ensure models respect clinical autonomy while strategically reducing administrative burdens where feasible. The lack of physician buy-in is a common physician alignment failure that can derail even the most well-conceived value models.
Contract Negotiation with Payers and ACOs
The successful execution of VBC strategy hinges on sophisticated contract negotiation, demanding deep actuarial insight and strategic foresight to manage risk and maximize value. The question, How should executives structure risk-bearing contracts profitably?, is central to financial stewardship in this evolving market.
- Sophisticated Financial and Actuarial Modeling: Developing robust internal capabilities to meticulously analyze potential risk, project cost savings, and forecast revenue under various VBC contract scenarios.
- Understanding VBC Contract Types: Possessing comprehensive expertise in navigating the nuances of various models, including shared savings, bundled payments, downside risk arrangements, and full capitation.
- Strategizing Risk-Sharing Arrangements: Negotiating favorable terms for both upside and downside risk, establishing clear performance guarantees, and defining quality metrics with payers to ensure equitable distribution of accountability and reward.
- Building Collaborative Payer Relationships: Fostering partnerships founded on transparency, shared goals, and joint problem-solving, moving beyond adversarial negotiation tactics to achieve mutual benefit.
Performance Metrics Beyond Traditional KPIs
To truly measure value, organizations must move beyond traditional volume-based Key Performance Indicators (KPIs) to embrace a more holistic and patient-centric suite of metrics. This is essential for C-suite accountability and transparency.
- Patient-Reported Outcome Measures (PROMs): Prioritizing metrics that directly reflect patient experience, quality of life, functional status, and overall satisfaction with care, shifting the focus to what truly matters to individuals.
- Total Cost of Care (TCOC) PMPM: Rigorously tracking the comprehensive cost per member per month across the entire care continuum to assess efficiency and identify areas for optimization. This provides a granular view of resource utilization.
- Population Health Indicators: Monitoring crucial rates such as preventable admissions, chronic disease management adherence, screening rates, and identifying and addressing disparities in care delivery. These metrics are critical for understanding and improving the health of entire communities.
- Utilizing Balanced Scorecards: Implementing comprehensive dashboards that integrate financial, quality, operational, and patient experience metrics for a holistic and nuanced evaluation of VBC program effectiveness. This allows population health metrics to effectively drive C-suite accountability.
Scaling Value-Based Models Across Enterprises
Achieving enterprise-wide adoption of VBC requires meticulous planning, standardized execution, and a commitment to continuous learning across diverse service lines and regions.
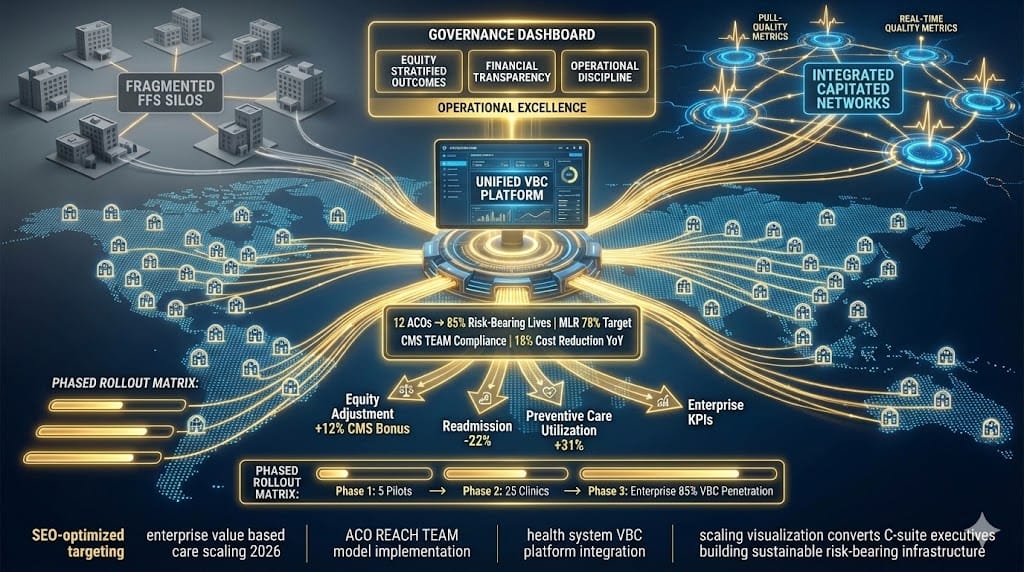
- Developing Standardized Playbooks: Creating replicable operational models, protocols, and best practices for VBC implementation that can be consistently applied across multiple service lines or geographical regions, ensuring fidelity to the model.
- Establishing a VBC Program Management Office (PMO): Centralizing oversight, strategic resource allocation, and coordination for all value-based initiatives, ensuring alignment with organizational goals and efficient execution.
- Leveraging Learnings from Pilots: Systematically capturing insights and best practices from initial VBC pilot programs to refine strategies, mitigate risks, and avoid common pitfalls during broader enterprise-wide rollout.
- Fostering Continuous Learning and Adaptation: Building robust organizational mechanisms for ongoing evaluation, feedback loops, and iterative improvement of VBC models, ensuring agility in a dynamic market.
In conclusion, the imperative to transition to value-based care models is undeniable and represents a core strategic challenge for executive leadership and boards today. The future success of US healthcare organizations hinges on their ability to cultivate a new generation of leaders who are not only financially astute but also deeply committed to patient outcomes, technological innovation, and sustainable population health. This requires a proactive approach to talent architecture and development. As we look ahead, the prevailing question isn’t if, but rather Will value-based models dominate healthcare economics by 2030? All indicators suggest an emphatic yes, underscoring the urgency for decisive and visionary leadership today.
FAQs: Executive Leadership in Value-Based Care
- What are the primary geopolitical drivers accelerating the shift to value-based care models?
- How can executive leaders effectively measure the ROI of value-based care investments in the short term?
- What role does artificial intelligence play in achieving population health goals within VBC?
- How can smaller healthcare organizations compete and thrive in a value-based care landscape dominated by larger systems?
- What steps should executive leadership take to mitigate financial risks when transitioning to capitated payment models?
As healthcare delivery networks navigate escalating operational costs and shifting federal reimbursement mandates, the transition away from volume-driven fee-for-service frameworks has become an economic necessity. At JRG Partners, we have seen that legacy administrative methodologies frequently fail to manage the risk-sharing complexities inherent in modern health ecosystems. To successfully bridge this operational divide and optimize clinical performance, healthcare organizations must prioritize identifying and securing specialized executive leadership for value-based care models. By embedding strategic visionaries who can align clinical quality metrics with cross-functional financial models, healthcare enterprises can accelerate risk-sharing adoption, eliminate structural inefficiencies, and reinforce long-term corporate effectiveness.

Tanya Gallardo
Managing Director, Executive Search & AI Talent Strategy
Tanya Gallardo is the Managing Director of Executive Search & AI Talent Strategy at JRG Partners, leading C-suite and Board engagements across key growth sectors including Technology, Financial Services, and Manufacturing.
With over 18 years of experience specializing in disruptive technology leadership, Tanya is recognized as a leading authority on talent architecture for future-focused executive roles, such as the Chief AI Officer (CAIO) and Chief Digital Officer (CDO). Her expertise lies in accurately assessing the cultural fit and technical depth required to ensure a high return on investment (ROI) for critical leadership appointments.
Prior to her role at JRG Partners, Tanya held senior roles directing global talent acquisition strategies at a major publicly-traded technology firm, advising on organizational design and succession planning for emerging executive functions. She is a recognized speaker and contributor to industry events, sharing data-driven insights on executive compensation, leadership development, and the measurable business impact of C-suite talent.